Zygomaticomaxillary complex (ZMC) fractures are the second most common facial fractures after nasal bone fractures. As plastic and maxillofacial surgeons, a strong understanding of the anatomy, patterns, evaluation, and management of these injuries is imperative for achieving optimal functional and aesthetic outcomes. This blog post provides a comprehensive overview of key considerations.
Anatomy
The ZMC defines midface width and projection. It is formed by the zygoma and 4 surrounding bones – frontal, maxillary, temporal, and sphenoid. It provides insertion points for the masseter, temporalis, and zygomaticus major/minor muscles and is closely associated with the infraorbital nerve.
Epidemiology
- Account for ~40% of midface fractures
- Second most common facial fracture after nasal bones
Pathology
- Direct blow to malar eminence
- Disrupts zygoma anchoring via 3 main fracture components
- Can cause trismus, infraorbital nerve injury/numbness
Evaluation
- History: mechanism, numbness, trismus
- Physical exam: 6 P’s of ZMC fractures
- Periorbital swelling
- Pain with gaze extremes
- Perception: diplopia, subconjunctival hemorrhage
- Paresthesia in V2 distribution
- Projection: lack of malar prominence
- Protusion: enophthalmos/exophthalmos
- Ophthalmology assessment: orbital apex syndrome, other ocular injuries
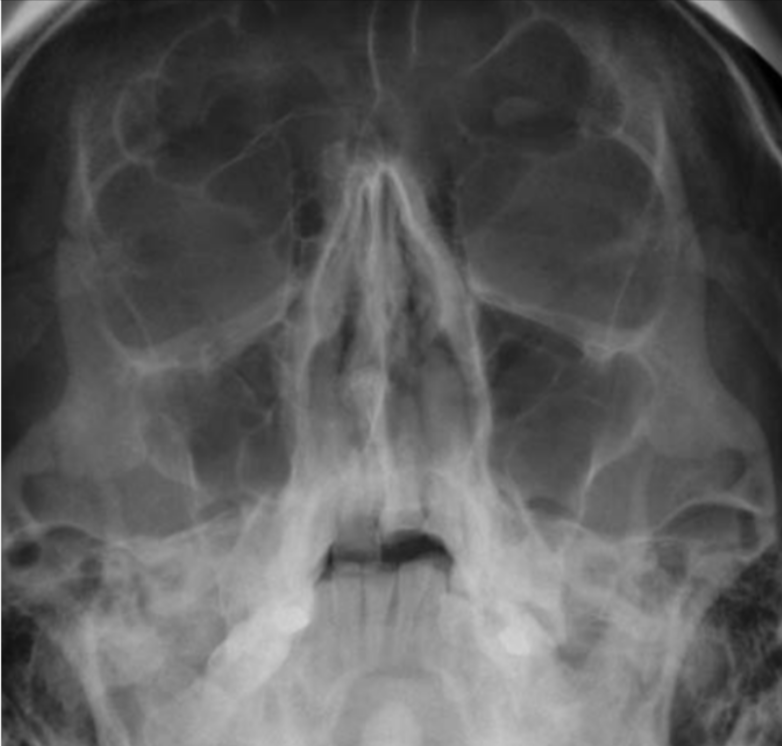
- CT scan with multiplanar reconstruction: gold standard imaging
Classification
- Zingg et al. 1992 classification:
- Type A: Incomplete zygomatic fracture
- Type B: Complete monofragment zygomatic fracture
- Type C: Multifragment zygomatic fracture
Management
- Goals: restoration of anatomy, function
- Closed reduction or open reduction/internal fixation
- Rigid fixation with plates, screws to stabilize fractures
- Soft tissue repair for coverage, aesthetics, ocular competence
- Timing: emergent if severe sequelae, otherwise delayed 1-2 weeks
The table below provides a summary overview:
| Characteristic | Description |
|---|---|
| Anatomy | Zygoma + 4 surrounding bones; associated muscles/nerves |
| Epidemiology | 40% of midface fractures; 2nd most common after nasal |
| Pathology | Direct blow to malar eminence; disrupts zygoma anchoring |
| Evaluation | History, physical, ophthalmology assessment, CT scan |
| Classification | Zingg: Types A, B, C based on fracture components |
| Management | Anatomical reduction; rigid internal fixation; soft tissue repair; timing |
References:
Ranchod, A. I. (2023, September 14). Zygomaticomaxillary complex fracture: Radiology reference article. Radiopaedia. https://radiopaedia.org/articles/zygomaticomaxillary-complex-fracture-1?lang=gb
PlasticsFella. (2021b, December 12). Zygomaticomaxillary complex (ZMC) fractures. thePlasticsFella. https://www.theplasticsfella.com/zygomaticomaxillary-complex-fractures/